While in Romania, I bought this amazing book: “Microbiomul: Sănătatea Începe în Intestin” by Prof. Dr. Maria Rescigno, in a Romanian translation of the original Italian book “Microbiota Geniale: Curare l’intestino per guarire la mente” (2023). I find the content very well explained to laypeople. The book is a fountain of new information that should interest all of us. The gut microbiome is considered a new organ that stays at the basis of human health. It is known that about 90% of all diseases start from gut microbiome dysbiosis. This book is available in English
The author, Dr. Maria Rescigno, PhD, a renowned biologist and researcher at Humanitas University, is recognized as one of the world’s leading experts on the microbiome. She has published over 200 papers in top journals like *Science* and *Nature*, and her groundbreaking discoveries include the gut vascular barrier (GVB) in 2015 and the plexal vascular barrier (PVB) in the brain in 2021. The book explores the intricate connections between the gut microbiome, the immune system, and the brain, emphasizing how modulating the microbiome can prevent and treat various health issues, particularly neurological and mood disorders.
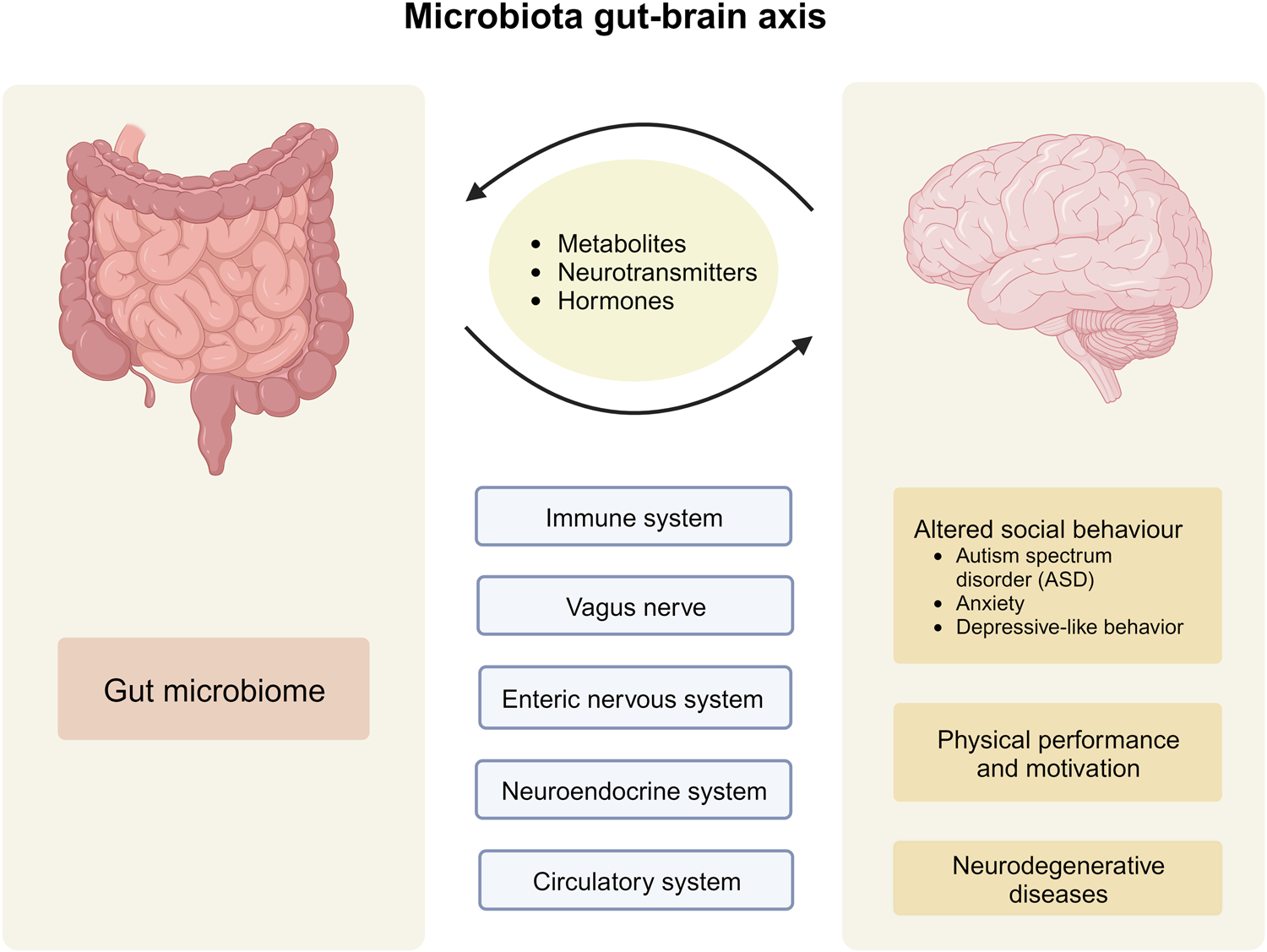
The central thesis is that health begins in the gut, where a rich population of microorganisms (the microbiome) aids digestion, communicates with the immune and nervous systems, and influences overall well-being. Rescigno highlights the bidirectional gut-brain axis, regulated by the microbiome, and draws from recent research—including her own—to show how imbalances (dysbiosis) in the gut can contribute to conditions like anxiety, depression, Alzheimer’s, Parkinson’s, autism, and eating disorders. The book combines scientific rigor with accessible explanations, offering practical strategies for microbiome modulation.

{kind=link}
Chapter 1: A Brief Excursion into the World of the Microbiome
This chapter introduces the microbiome as an “additional organ” composed of bacteria, viruses, fungi, and other microbes inhabiting our mucous membranes, particularly the gut. Rescigno explains its evolution from being called “bacterial flora” to “microbiome,” detailing its roles in metabolism, immune modulation, and communication with the body. She describes the microbiome’s diversity, likening the gut to “guest rooms” or “shores” where microbes interact with host cells. The chapter sets the stage for understanding how this microbial world impacts health beyond digestion.
Chapter 2: What Are Barriers and What Role Do They Play?
Rescigno delves into protective barriers in the body, focusing on the intestinal vascular barrier (GVB), which she discovered, and its similarity to the blood-brain barrier. She discusses intestinal permeability and leaky gut syndrome (LGS), where breaches allow harmful substances to enter the bloodstream. The chapter also covers the two brain barriers: the blood-brain barrier and the newly identified plexal vascular barrier (PVB) in the choroid plexus, which controls substances entering cerebrospinal fluid. Drawing on experiments, including those by researcher Michal Schwartz, Rescigno explains how these barriers open and close in response to gut-derived stimuli, forming a vascular gut-brain axis.
Chapter 3: The Two Brains
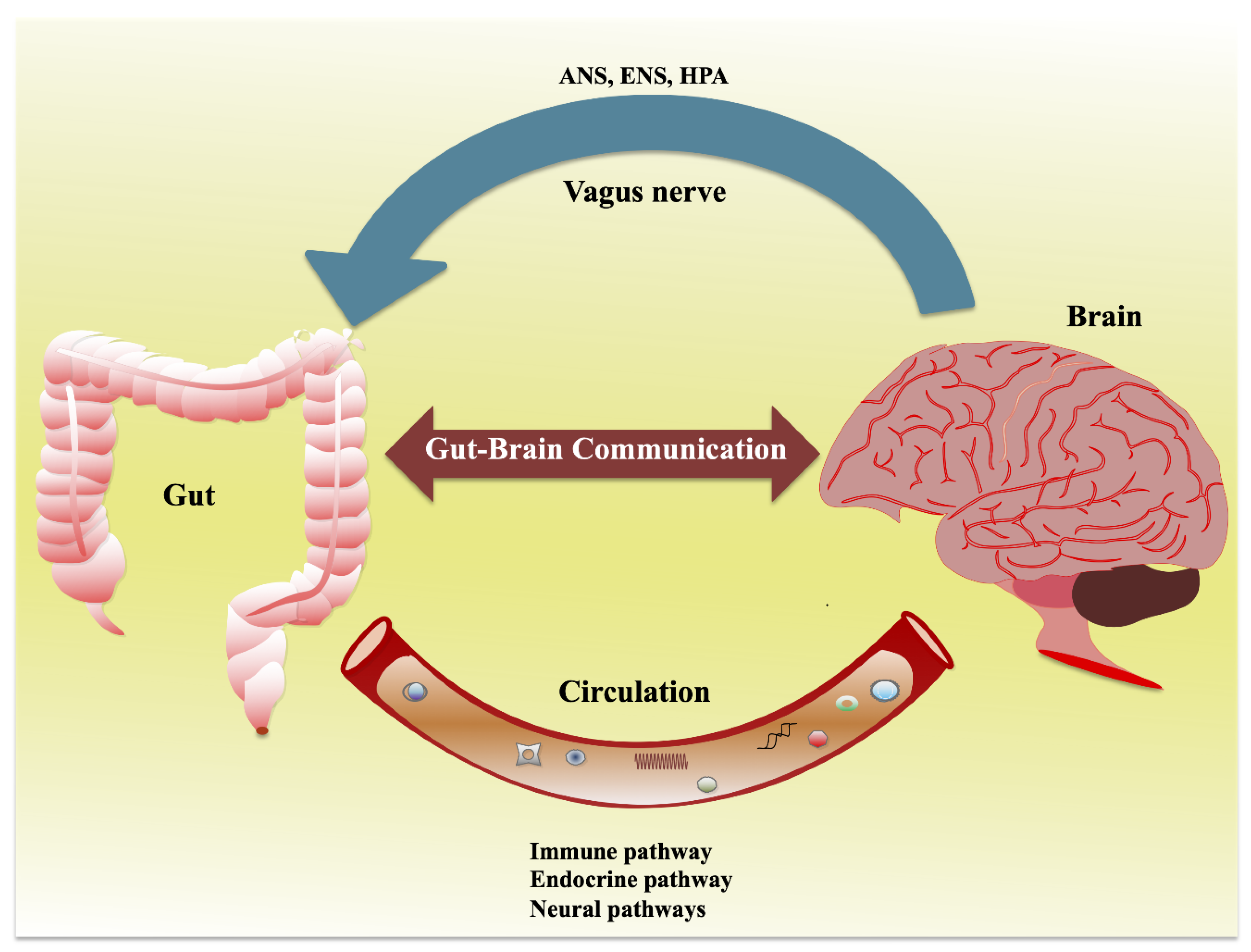
Here, the author explores the “second brain”—the enteric nervous system in the gut—which engages in constant dialogue with the central nervous system. Communication channels include the nervous system, vagus nerve, immune pathways, and hormonal signals. Rescigno details how microbes produce neurotransmitters and metabolites that influence mood control centers in the brain, acting as key players in this bidirectional exchange. She emphasizes that gut microbes can “write” messages that affect emotions and behavior.

{kind=link}
Chapter 4: Neurological Diseases and the Microbiome
This extensive chapter links microbiome dysbiosis to various conditions. It questions causality (“chicken or egg?”) and examines microbiome changes in aging, Alzheimer’s (involving microglial cells), Parkinson’s (gram-positive/negative bacteria), sleep issues (melatonin), ALS, multiple sclerosis, IBS, anxiety (including sepsis-related), depression (major and bipolar), schizophrenia, psychosis, and childhood/adolescent disorders like autism (role of bifidobacteria) and drug-related psychosis risks. Beyond the gut-brain axis, it touches on periodontitis and neurodegenerative links.
Chapter 5: The Microbiome and…
Focusing on eating behaviors, this chapter discusses satiety, eating disorders like anorexia, and how diet influences social behavior via the microbiome. Rescigno presents evidence from studies showing microbiome composition differs in patients with nutritional disorders, and maternal nutrition can shape offspring behavior through microbial mechanisms.

{kind=link}
Chapter 6: Prevention and Treatment of Neurological Diseases Through Approaches That Modulate the Microbiome
Rescigno shifts to actionable strategies, covering nutrition’s protective role against neurodegeneration. She highlights plant-based antioxidants like polyphenols, flavonols for Parkinson’s, Korean red ginseng for Alzheimer’s, ketogenic diets for IBS, olive/camellia oils, and omega-3s. The chapter reviews pre-, pro-, and postbiotics, clinical trials (e.g., Lacticaseibacillus rhamnosus for mood in overweight patients, probiotic mixes for depression and autism), fecal microbiota transplants, bacterial metabolites, and fermented foods like kimchi. Preclinical models and in vitro studies support these interventions.
Chapter 7: Future Perspectives
The book addresses limitations in microbiome analysis and offers practical advice: avoid leaky gut and high animal fat diets; consume fiber-rich foods, healthy fats, Mediterranean diet staples (legumes + cereals); prefer fermented foods; consider in vitro fermentation tests and postbiotics; try a 15-day grain-free test; and incorporate daily exercise. Rescigno discusses open research challenges and potential advancements in biomedical applications.
Conclusions
Dr Maria Rescigno concludes that modulating the microbiome through lifestyle and targeted interventions can preserve intestinal barriers, balance the gut-brain axis, and mitigate neurological risks, empowering readers to take control of their health.
**Citation:** Rescigno, Maria. *Microbiomul: Sănătatea Începe în Intestin*. Translated by Donna Oprea, Philobia, 2024. (Original: *Microbiota Geniale: Curare l’intestino per guarire la mente*. Vallardi, 2023.)